
When I first started this blog, it was intended to keep friends and family updated on my journey, but throughout the years this has also become a place where fellow ALK positive cancer survivors can learn to help inform their treatments as well. All this to say, the below may be very medically dense so be warned!
Last Thursday, I woke up bright and early at 4am to arrive in Charlottesville at 5:30am for the big procedure. I was the first case of the day so I expected to be in recovery shortly after lunchtime. Being the wonderful wife that she is, Varisara arrived in the recovery room with a bag full of pastries and bread because she knew I would be hungry after the surgery (which I was). She told me that she talked to Dr. Martin and the surgery went well – they removed the upper left lobe and a few lymph nodes as planned, but they also had to remove part of the lower left lobe unexpectedly as well because the disease appeared to be attached to the fissures between the upper and lower lobes. This caused a moderate volume pneumothorax, when air leaks into the space between the lung and chest wall, which meant that the chest tube would likely need to stay in for longer than I initially expected (I was hoping to be out of there in 2 days).

That afternoon, I generally felt ok but had a bit of brain fog and nausea, which I assumed was from the anesthesia medication. I pretty much just stayed in bed with my eyes closed for the afternoon, but I did chow down on some croissants, bread, and Sour Patch Kids hoping that all would somehow help the nausea. That night, I went to bed fine, but I woke up in the middle of the night to vomit twice, each time expelling over a liter of fluid.
The next day, they removed my foley catheter because they expected me to begin moving around to help with recovery – boy, were they wrong! I was no longer nauseous, but I was starting to feel the pain. Oddly, the pain was not in my chest; rather, it was in my abdomen. I didn’t eat much because of the pain and every time I took a sip of water, I felt very full. It gradually worsened throughout the day; my abdomen felt like it was getting more firm and it was getting harder to breathe as the day progressed. By mid-morning, breathing was incredibly difficult and my breaths became very shallow – so much that I could not talk or keep my eyes open. When I was originally diagnosed with cancer, I always feared that I would not live as long as my peers and that night, I felt that I was pushed to the limits and death or serious complications were about to occur. Over time the doctors grew more and more concerned and thought that it was strange that my pain level was at a 10 out of 10, but I felt no pain at the surgical site. They decided to do a CT scan to figure out what was going on.
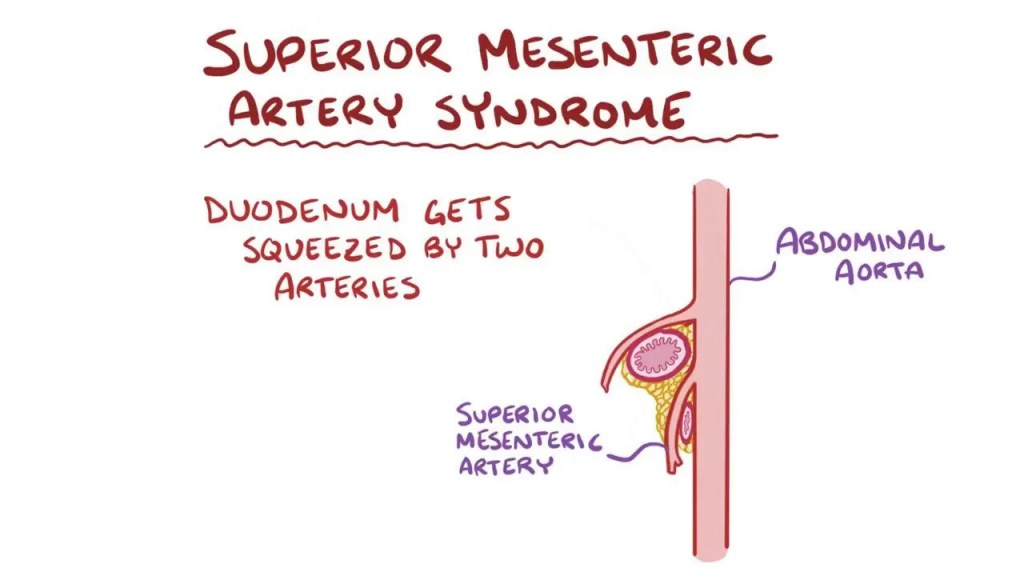
Radiology noted that the blockage appeared to be Superior Mesenteric Artery (SMA) syndrome, a digestive condition that occurs when the duodenum is compressed between two arteries (the aorta and the superior mesenteric artery). Traditionally, SMA syndrome occurs over a long period of time and is due to rapid weight loss. Personally, I don’t believe this was SMA syndrome because I had minimal weight loss (part of which was the lung that was removed) and the blockage occurred rapidly. I think the cause of the problem is very similar, but was rather due to my gastrointestinal system still being asleep from anesthesia when I rapidly consumed my food immediately after surgery. This as a post-operative complication was so bizarre that Dr. Martin said she had never seen something like this in her 20 years in practice.
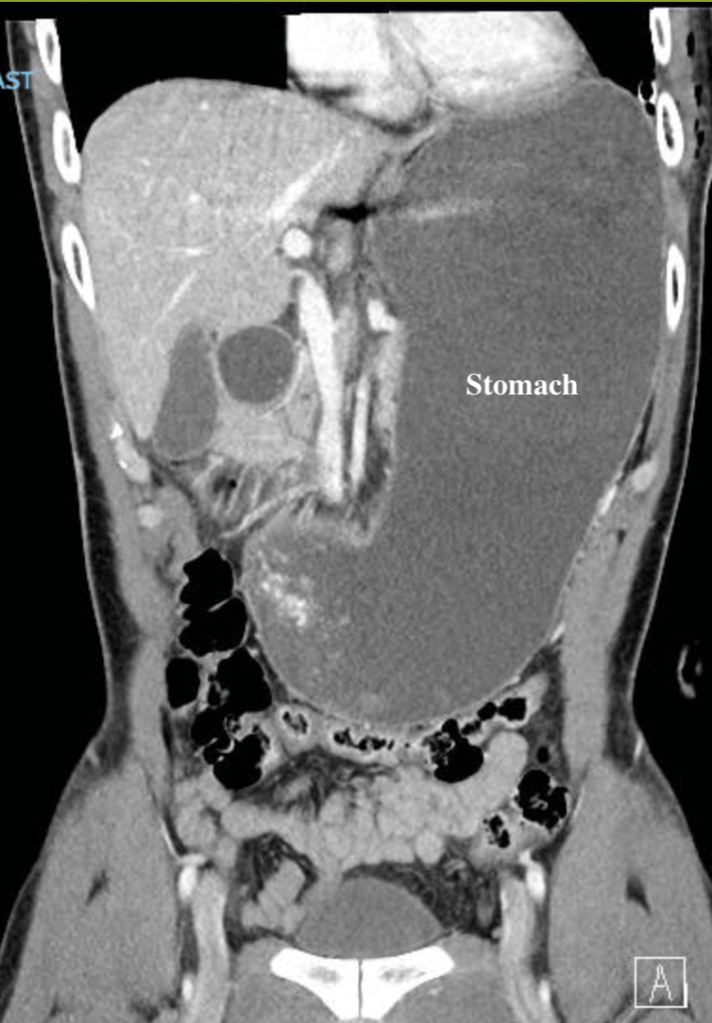
The obstruction in my duodenum caused me to be massively distended (and when I say MASSIVE, I mean it was the size of a watermelon). Now that we knew WHAT was wrong with me, we needed to figure out HOW to fix it. They immediately put in a nasogastric (NG) tube up my nose and down to my stomach to suction out the fluid. I was not allowed to eat or drink anything – not even a sip of water – until they were able to decompress my stomach. This included oral medications, which meant I had to stop taking Alectinib (my cancer medication) until this was resolved. They also had to reinsert the foley catheter to drain my bladder because of my decreased mobility (Pro tip: I would NOT recommend doing this awake if at all possible). At this point, going anywhere proved to be logistical challenge with a chest tube from the surgery, the NG tube, several lines of IVs and now a foley catheter.
They also discussed potentially inserting another tube into my intestines past the obstruction to pump food and nutrients into my body, but I already felt tethered to the bed due to all the other tubes and IVs. Fortunately, the Thoracic team consulted with the experts on the abdomen (i.e., the General Surgery team) to determine next steps. They suggested monitoring to see if my body could naturally alleviate the blockage and only recommended the nasogastric tube feeding only as an escalated alternative. We decided to drain the stomach for the next day, provide nutrition through Total Parenteral Nutrition (TPN), an intravenous method of feeding people by giving nutrients through an IV, and monitor for improvement.
For the next day or so, I was in pretty intense pain ranging from a 4 when I was heavily medicated (with Ketamine, Toradol, IV Acetaminophen, and Dilaudid) to an 8 when the medication wore off, but the pain was becoming more “normal” for the surgery that I had (i.e., the pain slowly shifted from my abdomen to the chest). In the one day that I had the NG tube suction in my stomach, roughly 4 liters of liquid was drained! Now with less liquid in my belly and a tolerable pain level, I knew that I needed to get up and walk around; not only to help the healing process for the lungs, but also to get my bowels moving so that my body could correct the obstruction spontaneously.
By Sunday, my surgical recovery for my lung was going relatively well. The pneumothorax had decreased in size since, which meant they were able to remove my chest tube as well as the foley catheter. This was a huge win and had it not been for the intestinal obstruction, I would have been discharged. Alas, I remained in the hospital – now with just 1 tube and multiple IV lines.

With the lobectomy recovery in a good spot, I focused my efforts on correcting the intestinal obstruction and reducing my reliance on medications administered by IV.
For the gastric (stomach) distension, we decided to clamp the NG tube for 4 hours to test the level of blockage. If the drainage was under an acceptable threshold (less than 250ML), then I would be able to start very slowly with small sips of water. After 4 hours, we drained 150ML from my stomach – well under the threshold – so I was finally able to have my first sips of water in 2 days. Talk about refreshing! Since I felt well after my water trial, they removed the NG tube and advanced my diet the next morning. Clear liquids was my Monday diet plan (I had lots of Gatorade, soup broth, jello, and more water). By Tuesday, my body seemed to be responding well to the clear liquids so I was advanced to a full liquid diet. By that evening, I was advanced to a transitional diet (very bland, easy to digest food) and I could start to see a light at the end of the tunnel.
All the while, I was slowly trying to transition myself to oral pain medications. When I was upgraded to a clear liquid diet, I transitioned to liquid Tylenol, ibuprofen, oxycodone. Then when I could have a full liquid diet, I was able to start back on my Alectinib after being off for 3 days and added Gabapentin (for pain) and Robaxin (muscle relaxer). By Tuesday night, I also transitioned off Ketamine and Toradol and was only using Dilaudid as needed when there were bouts of intense pain.
By Wednesday, I was back on a full diet and adequately managing my pain via oral options. I felt like I had made a complete 180 from where I was on Friday and thankfully the surgical team agreed – I was discharged that afternoon! When I went in, I thought I would be home by the weekend. Dr. Martin indicated that lobectomy patients typically stay in the hospital for 2-6 days and being young and relatively healthy, I expected to be out on the lower end of that range. Here I was 6 days later, but SO glad to be out.

Since being home, I’ve had some pain at my chest tube and incision sites and I’ve noticed that walking up and down stairs is a bit more difficult, but nothing unusual for having a quarter+ of my lung removed. I’ve felt great otherwise and I was even able to take Avery to her Kindergarten sneak peak 2 days after leaving the hospital! I know that recovery will take time, but I am just so glad that things are are starting to level out – I’ve had my fair share of excitement in the past 10 days.
